CARDIOVASCULAR DISEASES
PATENT DUCTUS ARTERIOSUS
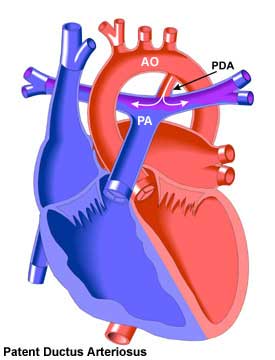
Patent ductus arteriosus is a connection between left pulmonary artery and aorta. It is a congenital disorder in the heart wherein a neonate's ductus arteriosus fails to close after birth. This connection is usually localized just below the left subclavian artery. It can be related with other congenital heart disorders but also can be present as an isolated defect.
This connection between the two main vessels is present before birth. It is usually closed spontaneously after birth. The closure rates are low in premature babies but subsequent spontaneous closure can develop in these babies. In mature term babies, if there is no spontaneous closure, subsequent closure is not usually seen. In these babies, a part of the oxygenated blood pass throgh the aorta to the pulmonary artery and this will increase the volume and pressure of the pulmonary artery. Left ventricular volume will be increased and due to this increment, left ventricle works much and fails gradually.
Presentations of adult patients with PDA include:
a) Small duct with no LV volume overload (normal LV) and normal pulmonary artery pressure (PAP) (generally asymptomatic)
b) Moderate PDA with predominant LV volume overload: large LV with normal or reduced function (may present with left heart failure)
c) Moderate PDA with predominant PAH: pressure-overloaded RV (may present with right heart failure)
d) Large PDA: Eisenmenger physiology with differential hypoxaemia and differential cyanosis (lower extremities cyanotic, sometimes left arm, too)
There is a potential risk of endarteritis but it seems to be low. Aneurysm formation of the duct is a rare complication and may even compress the left main coronary artery.
HOW TO DIAGNOSE?
Echocardiography is an important diagnostic tool for the diagnosis of patent ductus arteriosus. Transthorasic echocardiography (TTE) can demonstrate the connection between the pulmonary artery and the aorta. Transesophageal echocardiography can also be performed. However, aortography is the best method to diagnose and to clarify the type of PDA. During aortography, an important classification system developed by Krichenko is used. Although CT or MRI can also provide good results for the diagnosis, aortography is the best method. We are using TTE and aortography in our clinic in all patients with the suspicion of PDA.
How do we apply percutaneous transcatheter PDA closure?