CARDIOVASCULAR DISEASES
MITRAL VALVE STENOSIS
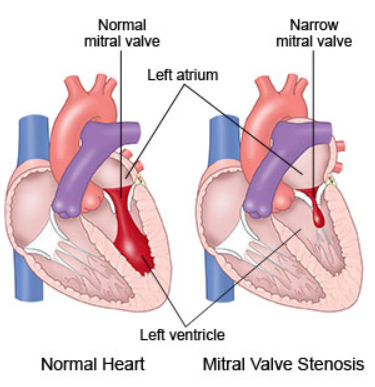
Mitral valve is a bicuspid valve which exists between left atrium and left ventricle. The dirty blood on the body comes to the right atrium and drop to the right ventricle. Right ventricle pumps the deoxygenated blood to the lungs. After the filtering period, the oxygenated blood drop to the left atrium. During the diastole, mitral valve is opened and the oxygenated blood pass through the mitral valve from left atrium to the left ventricle. During the systole, mitral valve is closed and the oxygenated blood will be pumped from left ventricle to the aorta. The reason of the closure of mitral valve during systole is to prevent the regurgitation of the blood to the left atrium. Normal mitral valve are is 4-6 cm2. If a stenosis will develop on mitral valve, the valve area will decrease and the drop of the oxygenated blood from left atrium to left ventricle will be difficult and the pressure in the left atrium will increase. This increase of left atrial pressure will be reflected to the pulmonary veins and to the pulmonary capillary arteries in which the blood is oxygenated.
Other rare causes of mitral stenosis: Congenital mitral stenosis (Parachute mitral valve, accessory mitral valve, fused papillary muscles, abnormal circular ring in left atrium), some connective tissue diseases such as Systemic lupus erythematosus (Libman Sacks endocarditis), Erosive polyarticular type of rheumatoid arthritis, some storage diseases (mucoploysaccharidoses, Fabry disease, Whipple disease), infective diseases (Fungal endocarditis), Heart tumours (Myxoma) and functional mitral stenosis due to severe mitral annular calcification or due to severe aortic regurgitation.
Usually there is no symptom until the mitral valve area decrease from its normal value to 2.5 cm2. However, if the valve area decreases less than 2.5 cm2, symptoms will develop gradually. First symptoms are usually fatigue and dyspnea. These symptoms are related inadequate filling of left atrium and reduced volume in the left ventricle due to the decreased mitral valve area and reduced forward volume to the aorta.
Due to the reduced filling of the left atrium because of the decreased mitral valve area, the blood will stay in the lungs and this situation will disturb the oxygenation and cause dyspnea. Dyspnea will first develop by hard efforts in mild mitral stenosis but will develop by minimal efforts in severe mitral stenosis.
If the valve area decreases to 1-1.5 cm2, this situation is termed as “moderate mitral stenosis”. If the valve area decreases below 1 cm2, severe mitral stenosis is developed. There can be dyspnea even at rest and effort capacity is markedly decreased. The patients can awake up on sleep with the complaints of dyspnea (Paroxysmal nocturnal dyspnea), open windows and try to breath and suppose to be in comfort by opening windows but the underlying reason for this comfort is related to decreased venous return of blood because of standing position. In the late stage, dyspnea on rest or sitting period is present and orthopnea is developed. The last stage is the pulmonary edema. In the pulmonary edema, blood and serum will pass through the capillary arteries to the alveolus due to increased pressure in the pulmonary capillary arteries and bubbly, wheezing or gasping sound during breathing, a cough that produces frothy sputum that may be tinged with blood will develop and the patient will be admitted to emergency service by these complaints. If the immediate therapy will not begin, the patient will be lost.
The increased pressure in the left atrium in mitral stenosis causes enlargement of the left atrium. If the left atrium enlarges, the duration of electrical activity will prolong and the normal cycle of electrical activity will be disturbed and a serious rhythm atrial fibrillation will develop. Atrial fibrillation itself also causes enlargement of left atrium and this vicious cycle will cause blood pooled in the left atrium. The viscosity of the blood in the left atrium will be disturbed and this situation will cause development of thrombus in the left atrium and in the left atrial appendage. A stroke can be developed due to the embolization of this thrombus to the systemic circulation. Sudden increases in the left atrial pressure can cause bleeding in the bronchial veins which drop to pulmonary veins and hemoptysis can develop. In some cases, hoarseness can develop due to the pressure of enlarged left atrium on laryngeal nerve.
Among patients who are not treated on the appropriate time period, the increase on left atrial pressure will be reflected to the pulmonary artery and due to the development of pulmonary hypertension, right heart failure will develop.
HOW IS MITRAL STENOSIS DIAGNOSED?
Echocardiography is an important diagnostic tool for the diagnosis of mitral stenosis. Transthorasic echocardiography clearly demonstrates the stenotic mitral valve. After calculation of mitral valve area by TTE, a transesophageal echocardiography is usually performed to clarify the degree of the stenosis, to demonstrate whether accompanying regurgitation to stenosis is present or not . TEE also examines the subvalvular apparatus and cleary identifies the presence or absence of thrombus especially in the left atrial appendage. After these examinations, an echocardiographic risk score is used to determine whether the mitral valve is suitable or not for the percutaneous therapy. Three D-TEE can also clearly show us the subvalvular apparatus and usually confirms us whether the valve can be treated without open surgery or not. We are using 3D-TEE in our clinic in all patients with the suspicion of mitral stenosis.
How do we apply percutaneous transcatheter mitral balloon valvuloplasty?