CARDIOVASCULAR DISEASES
PATENT FORAMEN OVALE
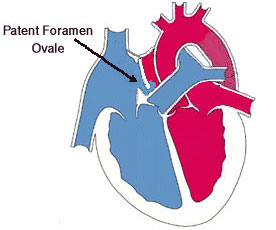
Foramen ovale is a valve like hole which is usually closed spontaneously after birth. In about 25% of adults, the foramen ovale does not close completely, but remains as a small patent foramen ovale (PFO) in the fossa ovalis region of atrial septum which is a layer between left and right atrium. In the general population, PFO already exists in one of every five persons and conditions that require PFO closure are less than 1%. In the presence of PFO, some conditions which increase intrathorasic pressure such as coughing, sneezing and valsalva open the valve like hole and there can be a shunt between left and right atrium. In some cases, the dirty blood in the right atrium does not go to the filtering system of lungs and pass through the PFO to the left atrium. In these situations, especially in patients with deep venous thrombosis, a clot in the dirty blood can pass through the PFO to the systemic circulation and can cause stroke and ischemic injury in some tissues.
There can be different types of PFOs in different persons. It has been postulated that some anatomical types of PFOs have increased risk properties for the development of stroke. These properties can be summarized as: large (>10mm) or long tunnel-type PFO, atrial septal aneurysm, prominent Eustachian valve (>10mm) and presence of right to left shunt at rest. If a PFO is detected in a patient with cryptogenic stroke, situations can be related to PFO closure can be summarized as:
a) Recurrent crytptogenic stroke despite traditional anticoagulation therapy
b) PFO associated transient ischemic attack, leg or coronary embolism despite anticoagulation therapy
c) Intolerance to anticoagulation therapy
d) Presence of a deep venous thrombosis in young age and PFO.
The clear relationship between migraine and PFO is not known. Thus, there is no sufficient data to close PFO in patients with migraine.
Platypnea-orthodeoxia is a relatively uncommon but a striking clinical syndrome characterized by dyspnea and deoxygenation accompanying a change to a sitting or standing from a recumbent position. It is usually seen in elderly patients and there can be some coexisting conditions in elderly such as aortic elongation, pneumonectomy, lung emphysema and liver cirrhosis. In these situations, upright position can cause displacement of vena cava and if there is a PFO, blood can be oriented to the vena cava superior and right to left shunt can be triggered. In these situations, PFO should be closed.
Routine systematic PFO screening is not recommended in astronauts, cosmonauts, miners and divers. However, screening could be considered for professional divers, in view of their frequent dives, and for deep and technical divers, given the higher risk of decompression lesions. In these risky persons, percutaneous closure should be individualized according to presence of symptoms, presence of high-risk anatomic features together with PFO, type and frequency of dives, and desire of the patient to continue with the activity.
HOW TO DIAGNOSE?
Echocardiography is an important diagnostic tool for the diagnosis of these defects. Transthorasic echocardiography makes a probable diagnosis but a definite diagnosis is made by transesophageal echocardiography. After detection of colour Doppler jets across the foramen ovale region by using 2D-TEE, real time 3D-TEE usually confirms the definite diagnosis. Three D TEE can also show us the location and the type of the defects and can confirm us whether the defect can be closed without surgery or not. We are using 3D-TEE in our clinic in all patients with the suspicion of patent foramen ovale.
How do we apply percutaneous transcatheter PFO closure?