CARDIOVASCULAR DISEASES
PULMONARY VALVE STENOSIS
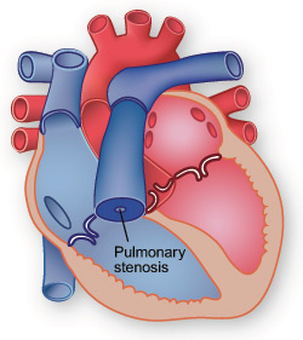
Pulmonary valve is present on the pulmonary artery which carries dirty blood from right ventricle to lungs. If a stenosis develops on pulmonary valve, afterload of the right ventricle increases and right ventricle works with a high pressure and force. In the course of time, right ventricle will enlarge gradually and right heart failure will develop.
Isolated pulmonary stenosis is always a congenital disorder and it is seen as 7-10% of all congenital heart diseases. Very rarely, carcinoid plaques, heart tumours or valsalva sinus aneurysm can cause pulmonary stenosis in adults.
In adults, the diagnosis of pulmonary stenosis is made according to its three type
a) Stenosis on the valve itself (valvular pulmonary stenosis),
b) Stenosis below the valve [subvalvular (infundibular pulmonary stenosis)],
c) Stenosis over the valve (supravalvular pulmonary stenosis).
In some cases, accompaniment heart defects such as ASD or VSD, some congenital heart disorders (Tetralogy of Fallot, Transposition of great arteries, Double outlet right ventricle) can bee seen with pulmonary stenosis. The most common type of the disease is valvular pulmonary stenosis. In these cases, leaflets are thickened, have deformities and the valve is a dome shaped due to the fusion of the leaflets. For this reason, the valve cannot open during right ventricular systole and right ventricle works under high pressure and force. Valvular pulmonary stenosis give not any symptom in the children except the neonatal period. In the adult period, due to the increased mass of right ventricle and because of right ventricular dysfunction, dyspnea, dizziness and syncope attacks can develop.In mild stenosis, the only sign is the murmur which is heard on pulmonary region. Some conditions which increase volume overload such as pregnancy can trigger symptoms.
The degree of pulmonary stenosis can be evaluated by the pressure gradient between right ventricle and the pulmonary artery. In mild to moderate stenosis, right ventricular pressure is less than the left ventricular pressure. However, in severe pulmonary stenosis, right ventricular pressure increases and can be higher than the left ventricular pressure. If there is a heart defect such as ASD in a patient with severe pulmonary stenosis, cyanosis can be seen.
The treatment of pulmonary stenosis can be managed according to the level and the degree of the stenosis and presence or absence of an accompanying congenital anomaly.
For the valvular pulmonary stenosis, the recommended therapy is percutaneous balloon pulmonary valvuloplasty however for the other types, repair by open surgery can be done.
HOW IS PULMONARY VALVE STENOSIS DIAGNOSED?
Echocardiography is an important diagnostic tool for the diagnosis of pulmonary stenosis. Two dimensional transthorasic echocardiography (TTE) can demonstrate the stenotic valve but the diagnosis is usually made by measuring the gradient accros the valve by continous wave doppler echocardiography. TTE can show the doming or dysplasia of the pulmonary valve. After calculation of pressure gradient by TTE, a transesophageal echocardiography (TEE) is usually performed to clarify the degree of the stenosis, to demonstrate whether accompanying regurgitation to stenosis is present or to examine the pulmonary annulus. The diameter of the pulmonary annulus is important for the balloon pulmonary valvuloplasty and it can be measured both by TTE and TEE. Three D-TEE can also clearly show us the pulmonary valve and can confirm us whether the valve can be treated without open surgery or not. Right heart catheterisation and measuring the peak to peak gradient is also important. By lateral right ventricular angiogram, pulmonary annulus can also easily measured. In our clinic, we use TTE, 2D-TEE and right heart catheterisation to confirm the diagnosis.
How do we apply percutaneous transcatheter pulmonary balloon valvuloplasty?