CARDIOVASCULAR DISEASES
VENTRICULAR SEPTAL DEFECT
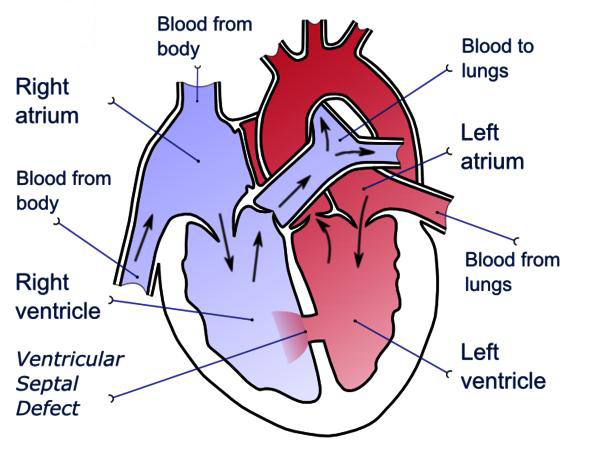
K There are two atrium and two ventricles in the heart. Ventricular septal defect is a congenital defect, a hole in the ventricular septum which is a layer between left ventricle and right ventricle.
Types of VSD
a) Perimembranous/paramembranous/conoventricular (most common, 80% of VSDs; located in the membranous septum with possible extension into inlet, trabecular or outlet septum; adjacent to tricuspid and aortic valve; aneurysms of the membranous septum are frequent and may result in partial or complete closure)
b) Muscular/trabecular (up to 15–20%; completely surrounded by muscle; various locations; frequently multiple; spontaneous closure particularly frequent)
c) Outlet supracristal/subarterial/subpulmonary/infundibular/supracristal/conal/doubly committed juxta-arterial [5%; located beneath the semilunar valves in the conal or outlet septum; often associated with progressive aortic regurgitation (AR) due to prolapse of the aortic cusp, usually right]
d) Inlet/AV canal/AVSD type (inlet of the ventricular septum immediately inferior to the AV valve apparatus; typically occurring in Down syndrome).
e) Post myocardial infarction VSD (VSD after heart attack): Typically occurs in patients with acute myocardial infarction and who did not take thrombolytic therapy or who did not undergo primary PCI. It is usually localised in the muscular septum. If the hemodynamic disturbance is present, emergency treatment is required. The first choice of treatment is surgery however it is very hard to put sutures on the necrotic area. Device therapy is the second choice but success rates are low in published series. If there is a chance to wait one or two weeks, device therapy can provide an important advantage to surgery.
The most common types of VSDs are perimembranous and muscular type defects and they can be closed by percutaneous transcatheter method without surgery. In past, the only treatment modality for perimembranous and muscular type VSD closure was open heart surgery but today, we can close them with special devices in the cath lab without open surgery. For the other rare types of VSD, we stil offer surgery.
HOW TO DIAGNOSE?
Echocardiography is an important diagnostic tool for the diagnosis of these defects. Transthorasic echocardiography usually confirm the diagnosis. Transesophageal echocardiography is also a useful tool especially for perimembranous defects to measure the distance between VSD rims and aort valve. After detection of colour Doppler jets across the ventricular septum by using 2D-TEE, real time 3D-TEE usually confirms the definite diagnosis. Contrast ventriculography is also an important diagnostic tool for us to confirm the distance between VSD and aort valve and to see whether aneurysm is present or not.
How do we apply percutaneous transcatheter ventricular septal defect closure?